The Canadian Paediatric Society on Tuesday announced that Dr. Natasha Johnson, a pediatrician and adolescent medicine specialist at McMaster Children’s Hospital in Hamilton, Ontario, would serve as its 2026 to 2027 president.

The announcement prompted immediate outcry on social media from critics of pediatric gender medicine, given Dr. Johnson’s position as a leading Canadian provider of gender-transition interventions to minors at the McMaster gender clinic she directs.
I’ll cover Dr. Johnson’s appointment in greater detail in an article I’m working on for next week. (If any experts out there want to comment for such an article, or if you have details that might help with my reporting, including suggesting people to contact, please get in touch.) But for now, I’ve published in this Substack a short conference presentation that Dr. Johnson gave at the 2022 World Professional Association for Transgender Health, or WPATH, conference.
Most notably, Dr. Johnson leveraged research about outcomes among youth attending gender clinics to assert that parents’ concerns about consenting to such treatment for their children should take a back seat to the youths’ preferences.
This conference video is one of over 100 that I viewed for my reporting about WPATH in Contact magazine. I am in the process of publishing these videos on my Substack. To see the full collection that I’ve published so far, visit:

The 2022 WPATH conference took place immediately after the organization published its long-awaited, much ballyhooed update to its transgender-care guidelines, known as the Standards of Care, Version 8, or SoC 8. So in her presentation, Dr. Johnson was taking issue with certain elements of the adolescent chapter of the SoC 8 in particular.
In short, she relayed that the Canadian youth attending gender clinics in her and her colleagues’ study did not undergo what she referred to a “a battery of psychological testing to verify their gender identity.” Nevertheless, she reported, two years after first presenting at the clinics, none of the youth who underwent gender-transition treatment significantly regretted it. She presented this to suggest that the SoC 8’s demands for how to assess these youth seeking gender-transition treatment were excessive and burdensome.
Dr. Johnson presented her data with Julie Temple, an adjunct professor of gender studies at Memorial University in St. John’s, Newfoundland. Neither of them suggested that their findings about treatment regret might be limited by the drop-off in youth providing survey responses at the two-year mark, or by the limited follow-up time. Research on detransitioning is notoriously sparse. But experts generally report that it can take several years or more for any treatment regret to sink in. Consequently, the two years of follow-up in this study would be unlikely to fully capture any ultimate regret that the cohort of youth might experience.
The presentation considered an analysis of data from the Trans Youth Can survey study, of which Dr. Johnson and Dr. Newhook were each coauthors. Their presentation at the WPATH conference was meant to “inform SoC 8 revisions.”
Dr. Johson expressed concern that, as she saw it, “the statement in the Language and Statement 11” of the SoC 8’s adolescent chapter “prioritizes the perspectives and worries of parents over the lived experiences of youth, and introduces additional barriers to accessing gender affirming care.”
Dr. Johnson also expressed concern that “Statement 12b requires youth to demonstrate several years of gender incongruence, verified through comprehensive psychosocial assessments, to access gender affirming care.”
Regarding assessments of youth seeking gender-transition treatment, she suggested that specialists are not necessarily needed for this. This was part of a larger theme at WPATH conferences of pediatric gender medicine specialists pushing for greater access to these treatments by suggesting they could be provided through primary care clinics.
“We want to emphasize that this can be done,” Dr. Johnson said of gender-transition treatment for minors, “by a variety of health care professionals, as was the case for youth in the trans youth can study.”
“The recommendations in both statements 11 and 12b,” she said, “seem based on the unproven presumption that youth accessing gender-affirming care are experiencing harm and regret in significant numbers that would be sufficient to restrict access to care for trans youth. Our participant participants, in fact, did not demonstrate such regret over a two-year period.”
Dr. Temple was among the multiple presenters at the WPATH conference sessions I have reviewed who disparaged or otherwise sought to discount the hypothetical phenomenon of rapid-onset gender dysphoria, or ROGD. She referenced a paper her team had just published in The Journal of Pediatrics and said that “the negative mental health outcomes that were proposed by the theory of rapid-onset gender dysphoria do not vary based on the time that youth knew their gender.”

The Trans Youth Can study, Dr. Temple said, included 174 youth who had already started puberty and were age 15 and older at 10 gender clinics across Canada. They were recruited at their first medical appointment at their respective clinics.
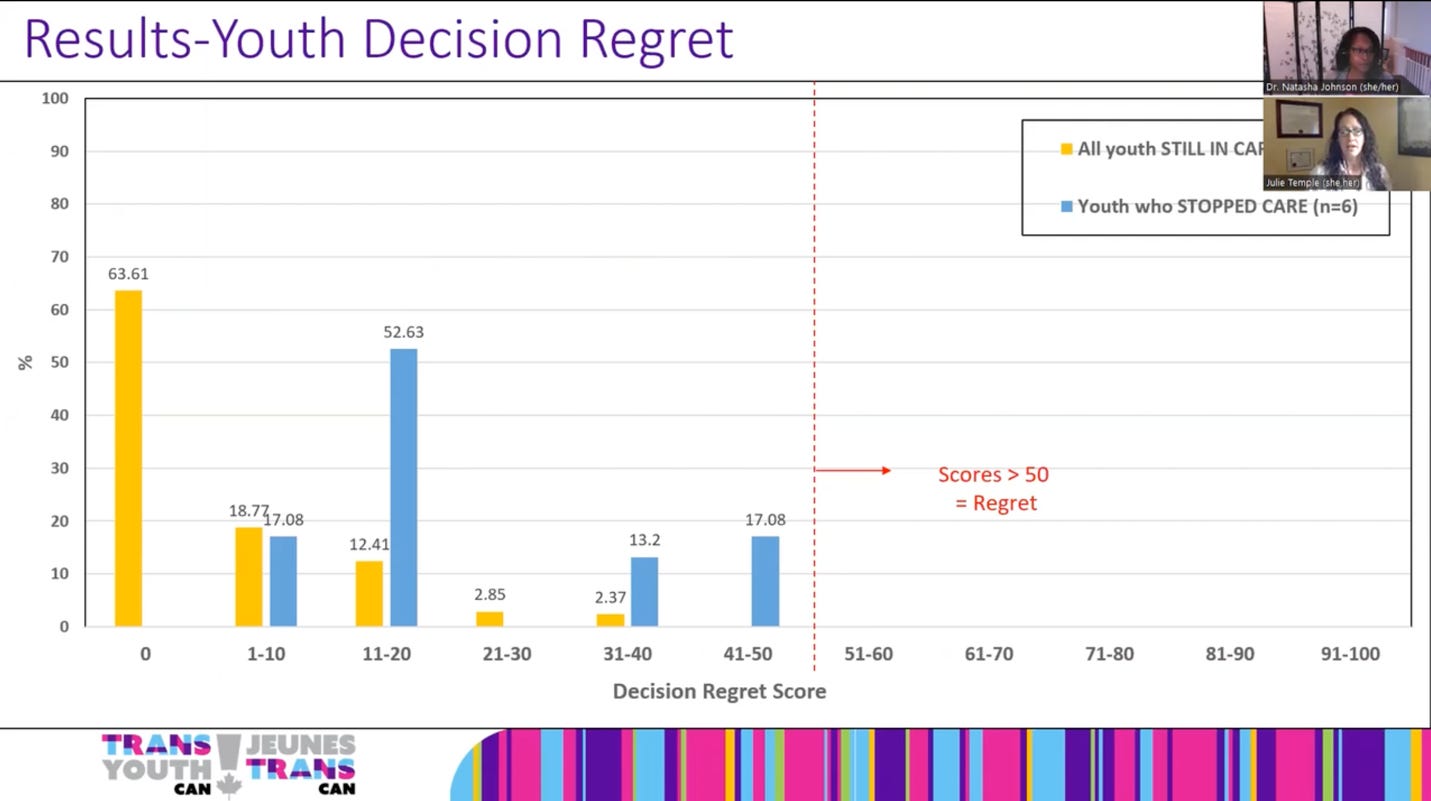
Dr. Temple said of the study design: “We included clinical medical records and short online symptom checklists for parents. Our measures included checklists of worries and positive feelings about their youth; gender for adolescence; for parental support for their gender-affirming medical care for both parents and adolescents. They completed a two-year follow up, a decision regret scale, including five items scored from 0 to 100, with scores above 50 indicating regret.”
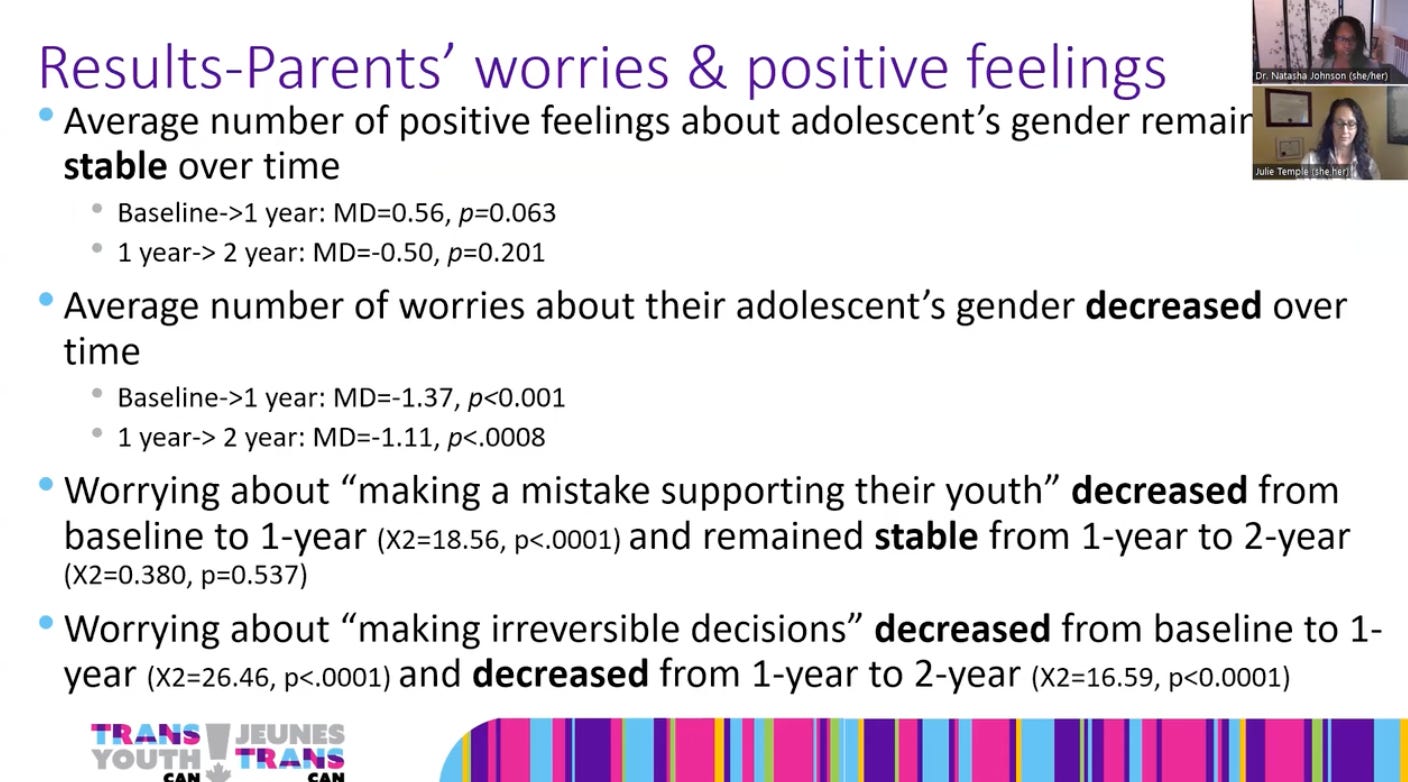
The study, Dr. Johnson said, found that parents’ positive feelings about their children’s gender identity generally remained stable over time, while the worries decreased. In particular, their worries about making irreversible decisions about gender-transition treatment decreased.
The youth, meanwhile, reported that support from their parents about their gender-transition treatment increased over time. At the first visit, 55 percent of the youth reported that their parents were very supportive of gender-transition treatment, a figure that increased to 69 percent two years later. (Note that the study as presented at the conference did not measure when these youth actually started treatment.)
Dr. Temple pointed to a diagram of the youths’ expressions of regret about their decisions about treatment. None of the youth expressed regret that crossed the threshold indicating significant regret. Note that only six of the 174 youth stopped treatment. That means that the two-year mark only included survey responses from 122 of 168 youth who went through with treatment—a response rate of just 73 percent, which went unmentioned. Did the 27 percent of youth who did not respond to the year-two survey regret their treatment? There is no information on that.
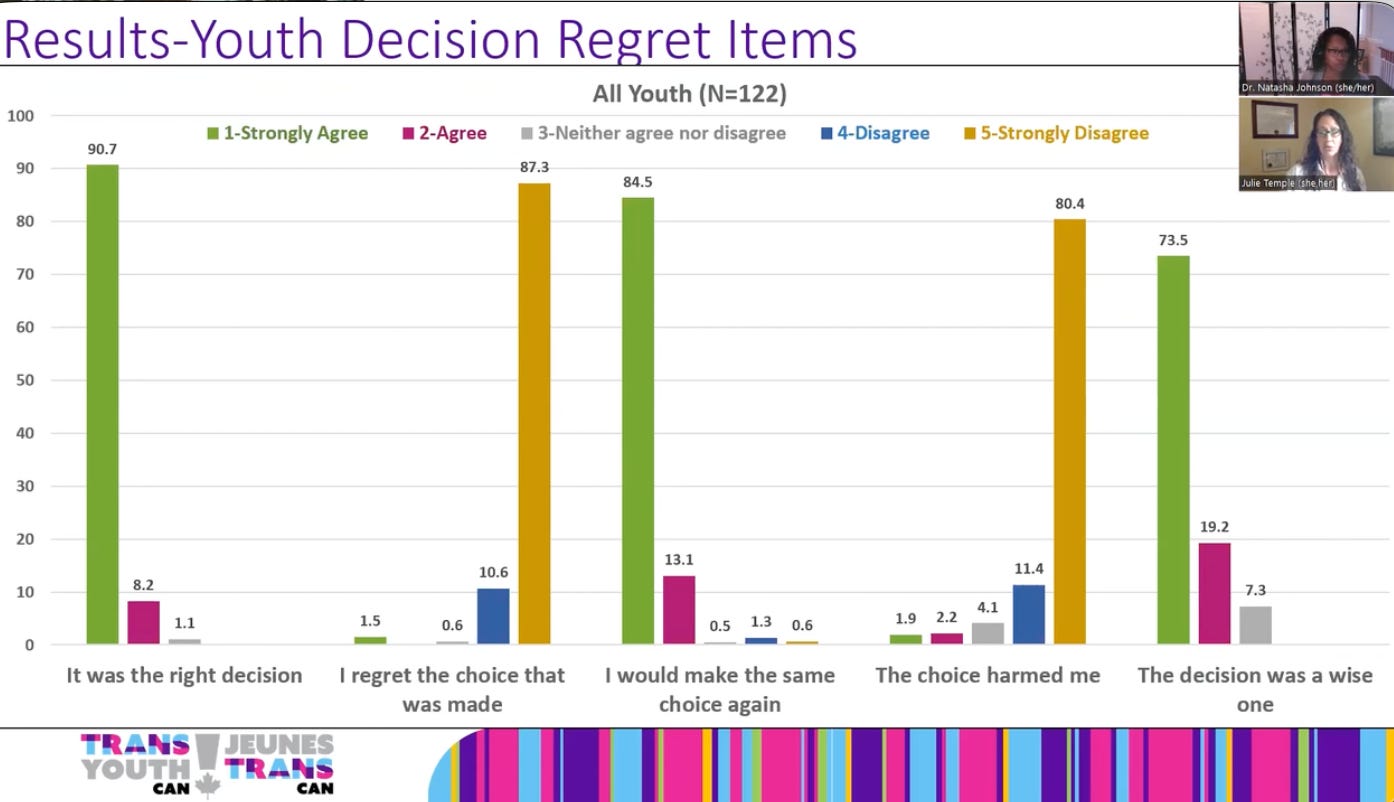
These were the five questions the youth were asked:
It was the right decision.
I regret the choice that was made.
I would make the same choice again.
The choice harmed me.
The decision was a wise one.
As you can see, of the 122 youth who responded to the survey at the two-year mark, they overwhelmingly endorsed answers suggesting that they did not regret their decision to undergo gender-transition treatment.
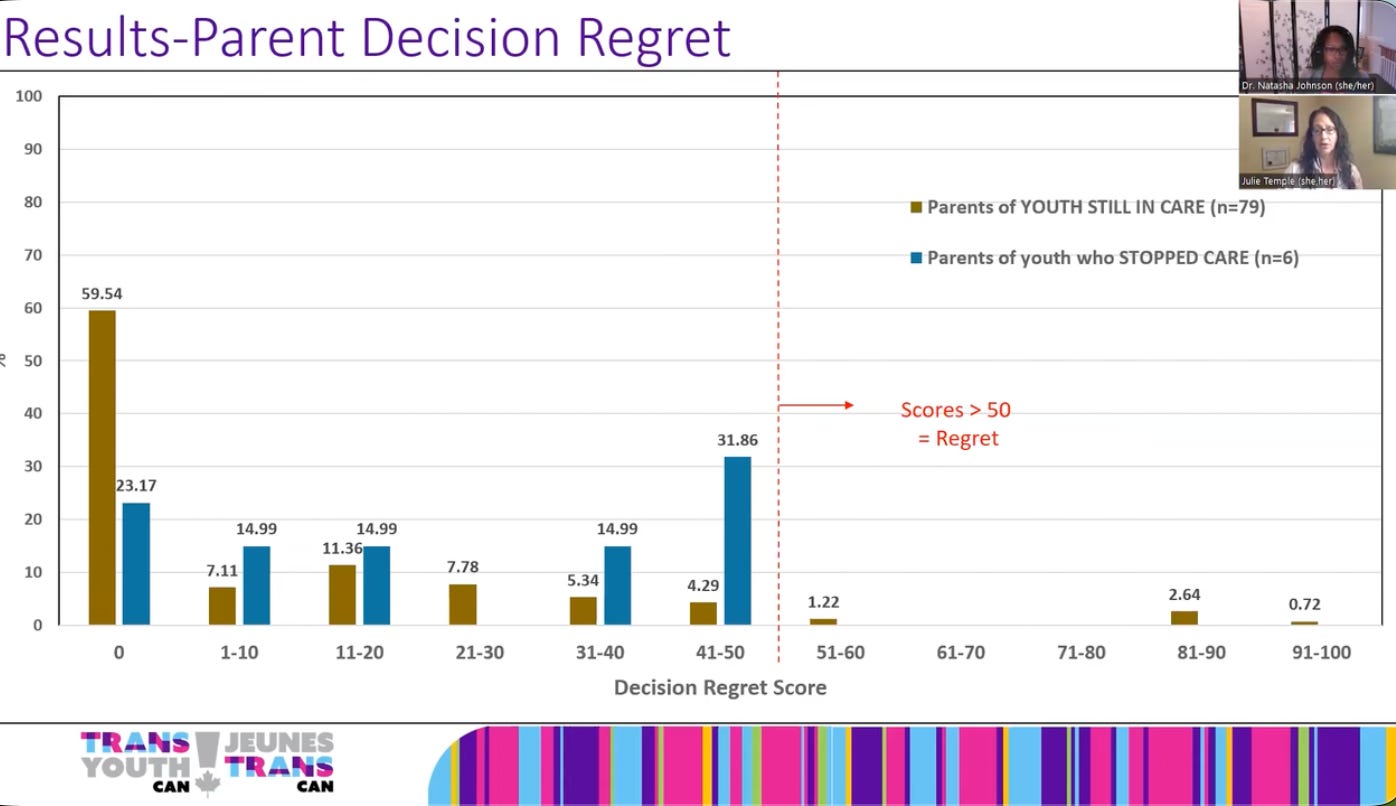
At the two-year mark, only three parents passed the threshold for regret on the scale.
Dr. Temple said: “The two parents you see here who had scored 90 and 95,” indicating very strong regret, “these were not parents whose regret was based on their youth’s experience. Instead, these were parents who had expressed regret right from baseline that they were against gender affirming care, and those feelings did not change. This is in spite of the fact that their youth did not express regret about gender-affirming care, and had continued to receive care.”
“So in conclusion,” Dr. Johson said, “youth in the Trans Youth Can study did not undergo a battery of psychological testing to verify their gender identity. Overall, there was minimal regret for parents and no regret for youth. Parents’ worries decreased over time and their support for their youth increased.”
Most notably, Dr. Johson concluded: “This suggests that parents feelings should not be prioritized over the youth’s experiences” when deciding whether to start minors on gender-transition medications. “There is no evidence to delay care based on the initial feelings of parents, given how their worries decreased over time and support increases.”

It is worth noting that this was a small study and there were only tiny numbers of parents who objected to gender-transition treatment. So it would have been impossible to detect a statistically significant signal of any association between parental objection and youth regret.
Otherwise, Dr. Johnson’s argument that parental objection should be deprioritized is framed solely from the youth’s point of view, based on a single variable: whether the youth regretted treatment two years after presenting at the clinic. The study did not consider other, more objective variables, such as whether the youths’ fertility or sexual function were apparently compromised, and whether those outcomes were associated with parental objections.
Nor did Dr. Johnson note that there may have been a selection bias at play, with more supportive parents tending to take their children to these particular clinics. Thus, the study would not have been able to capture the full breadth of parental feelings about youth seeking gender-transition treatments, or the other medical or psychological experts that families might have sought out to inform them about such treatment and possibly provide it.
This is also only a single data point, but it is worth noting that Claire Deacon, the mother of Fox Varian, the detransitioner who recently won a $2 million jury award after suing her psychologist and the plastic surgeon who performed her mastectomy when she was 16, was always opposed to the surgery. Ms. Varian did not openly admit that she regretted the surgery until three years later.

I am an independent journalist, specializing in science and health care coverage. I contribute to The New York Times, The Guardian, NBC News, The Free Press and The New York Sun. I have also written for the Washington Post, The Atlantic and The Nation, among many others. Follow me on X: @benryanwriter. Visit my website: benryan.net








I'm glad that Johnson is saying what lots of her colleagues and allies believe but are loathe to admit openly; they think youth should be able to transition when they want, in the way they want, and without regard for their parents' wishes or what WPATH says. In public they say no children are receiving surgery, parents are always involved, there are standards of care, but that's not how they act, and I don't think it's what they want.
“Enquête”, is a Radio-Canada investigative journalism program that conducted a clandestine recording of a 14-year-old girl on her first appointment to a gender clinic in Montreal. The episode was call "Trans Express". The girl in the video was given a prescription for wrong-sex hormones and it was suggested she consider a mastectomy. It took nine minutes. No parents were involved. The investigation recreated the scenario which led to other girls profiled in the program who actual went through this pathway including having the mastectomy completed. Barely out of high school one 18 year old girl was on crowd funding raising the money to get breast reconstruction. This is pretty sick stuff. This is the background story published 29 Mar 24:
https://presse.radio-canada.ca/television/13109/trans-express-a-enquete-demain/
Thank you Ben, Astounding. The loss to follow up is such an inconvenient truth for research in this area. No shock – it is not even mentioned. When we see that 122 of 168 youth responded, the need for clarification in the follow-up is obvious. Let’s start with: are they still alive? This is such a profoundly flawed approach to determine proper healthcare interventions.
I will digress here for a moment regarding this absurdity. Right now, the publicly funded healthcare system in the province of Ontario is covering the costs for an individual that wants a “front hole to go with this person’s pole”. Yes, that lifesaving medically essentially surgery known as “Penile Preserving Vaginoplasty” is covered at taxpayer expense in Canada. What medical need does this address - where does ones creativity end? As with the whole youth gender medicine façade, just because we can do something surgically to an individual does that make it necessary or provide a basis for offering it?
https://nationalpost.com/news/canada/ohip-coverage-penis-sparing-vaginoplasty
Honestly I feel that atleast some of these people are just straight up homophobic and horrified that a child could grow up to be homosexual.
I find my self open-mouthed with absolute disgust at the gung-go attitude of this supposed medically trained individual. One can only try to guess at what can possibly have convinced her to abandon every psychological/ethical precepts she must have learned at medical school, and every biological fact too. But let’s have a go anyway…
We don’t allow minors to smoke, drink alcohol, have sex, drive cars, fly planes, own guns or even leave formal education - but these horrifyingly brain-fuzzed people are suggesting that young teen should have their youthful flights of fancy, all pretty much driven by the gender woo activists on social media, affirmed without question.This whole thing smacks of money. There are some very rich, very powerful, very middle-aged, fetishist transvestite men who are driving this. They have infiltrated every institution and organisation in Canada, and carefully drip-fed the idea that men’s sex fetishes should be affirmed and ‘celebrated’. It’s grotesque. And what really makes me heave is that it’s the silly gullible “be kind” women who are being used by these men to push this fantasist’s sex agenda. They all know very well that they can’t change sex, but they really love the arousal they get from pretending.
But they don’t ‘pass’, so for them it would have been perfect if they could have had all this affirmation way back. Except that ‘way back’ they hadn’t really reached the level of porn-sickness that they attained by the time they were in their 50s, so they have to pretend they knew since they were 4 or 5. (It’s always 4 or 5, because a child that young is a vulnerable little thing and so the adult fetishist can use that to ramp up how own ‘poor little me’ act. So getting kids into the game is ideal, because it affirms these adult men even more, and they feel justified in their drive to bring their sex fetish out into the public arena.
‘Gender’ is just another word for stereotypes, and boy these men are all over the stereotypes. Apparently, to be a woman, you have to have long hair, make-up, lots of dinky dangly jewellery, a nice frock, a cutesy little baby nose and of course a pair of lovely tits. This is the only type they seem to want to be - because it’s a stereotype. Where are all the womanface men with tiny breasts & big noses, wearing sweatshirts, jeans & baseball caps? Nowhere of course, because they’re not ‘proper’ women to these mother-infatuated, sex-obsessed blokes.
It is a sad and truly depressing thing that women like this ludicrous Doctor’ Johnson have fallen for the male story hook, line & sinker. And it seems that all our mothers’ and grandmothers’ efforts to get out from under the idea that we must always please men and do what they say have been for nothing. Even though the very fact that little Natasha can be a doctor at all is because of all those women who fought for her right to do that.
I can only assume that she and others like her have had so much money waved in their faces, and so much intimidation from activists if they so much as make a peep against these men, that they chosen for their own enrichment to subsume their self-respect - and their very humanity - in order to betray their own sex.
To think that they actually believe this travesty of truth & reality is surely insupportable.